Anatomy
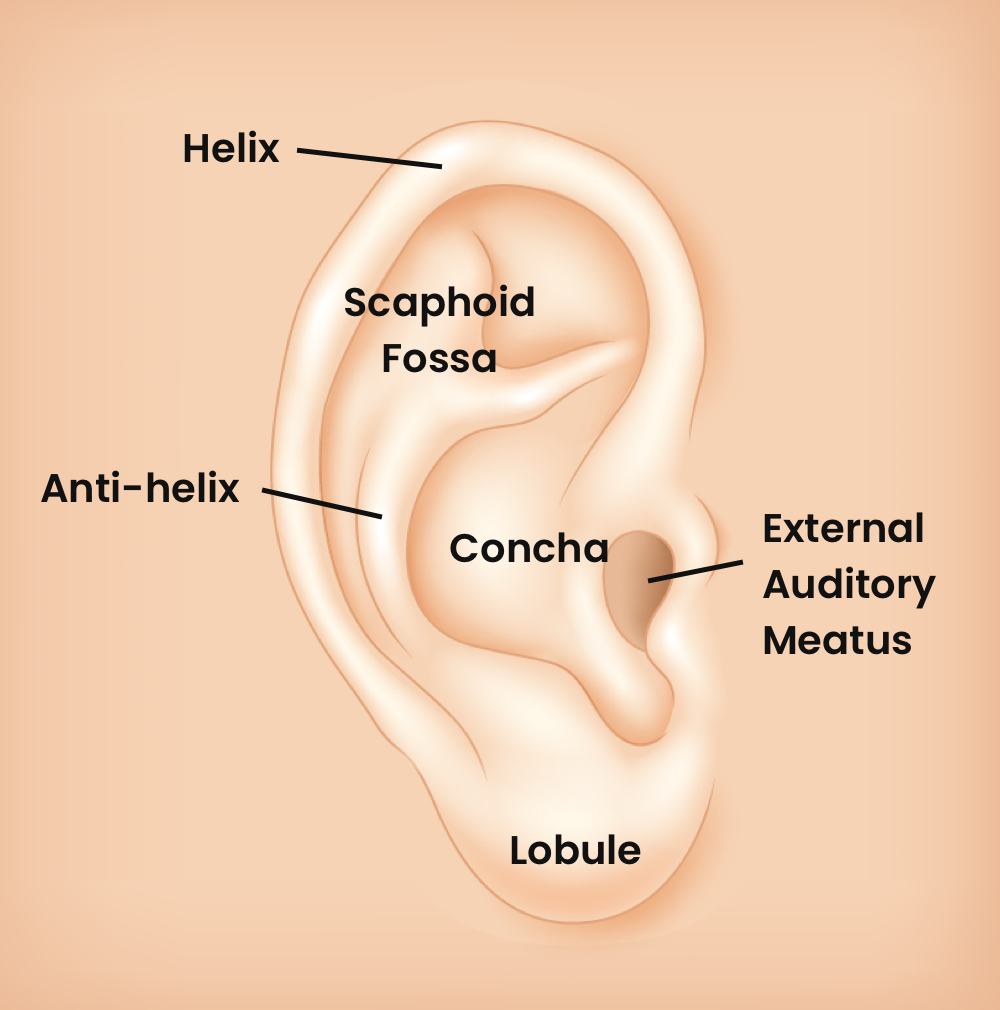
Landmarks and ear anatomy
Principles of Repair
- Cover the cartilage: the cartilage is avascular and derives its blood supply from the skin overlying it. Thus, it is critical to ensure the cartilage is covered to ensure its integrity.
Technique for improving wound margins.
- Optimize wound margins: For very macerated wounds along the helix, it is acceptable and sometimes advisable to perform a small triangular tissue wedge excision in order to create “surgical” wound margins that can be better approximated. Approximately 5mm of cartilage can be removed from this area without causing significant deformity.
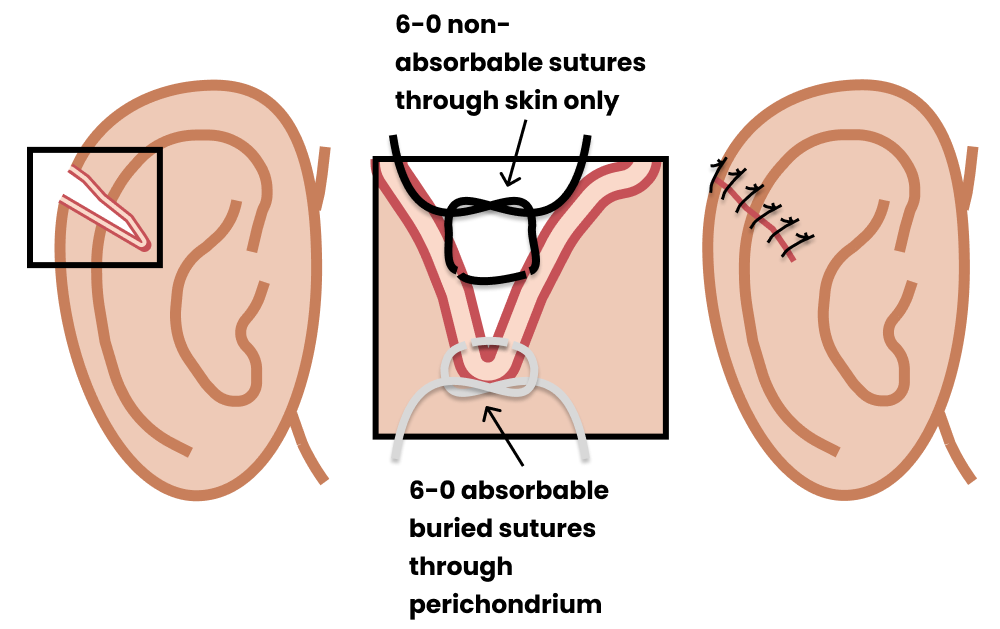
Technique
- Close the cartilage with simple interrupted deep dermal sutures using size 6-0 absorbable suture.
- Use the outer cartilage layer, the perichondrium, rather than piercing the mid-portion of the cartilage which is more fragile and prone to tear.
- Close the skin starting with the less noticeable posterior aspect of the ear with simple interrupted sutures using size 6-0 non-absorbable suture.
Auricular Hematoma Prevention
Even with a meticulous repair, the development of an auricular hematoma remains of concern. Hematoma formation associated with an ear injury can lead to separation of the cartilage from the overlying perichondrium, which can in turn lead to deforming neo-cartilage formation – commonly known as “cauliflower ear.”Gauze Packing

Image from Mohseni, Michael & Szymanski, Theodore. (2019). Acute Non-Traumatic Spontaneous Auricular Hematoma. American Journal of Case Reports. 20. 204-206. 10.12659/AJCR.913464.
Plaster Packing
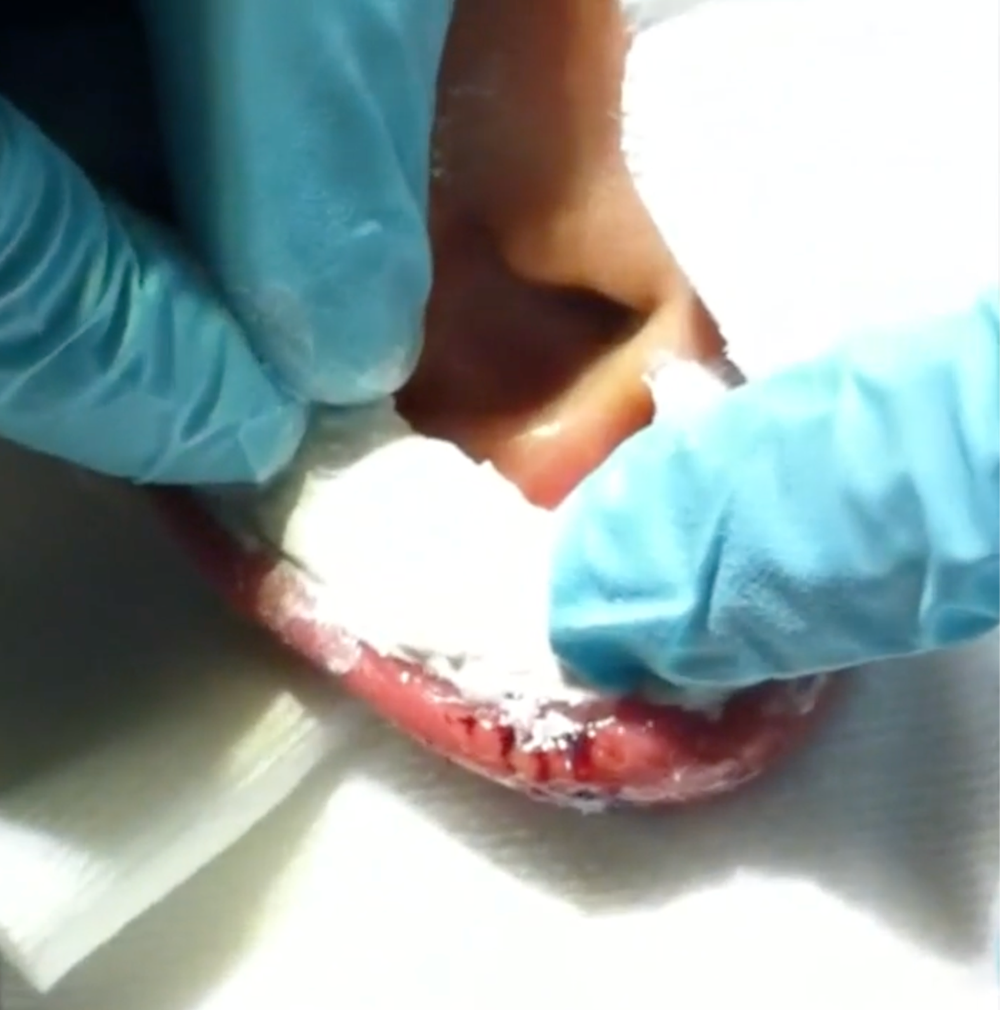
Image from Closing the Gap